What is the A-a Gradient?
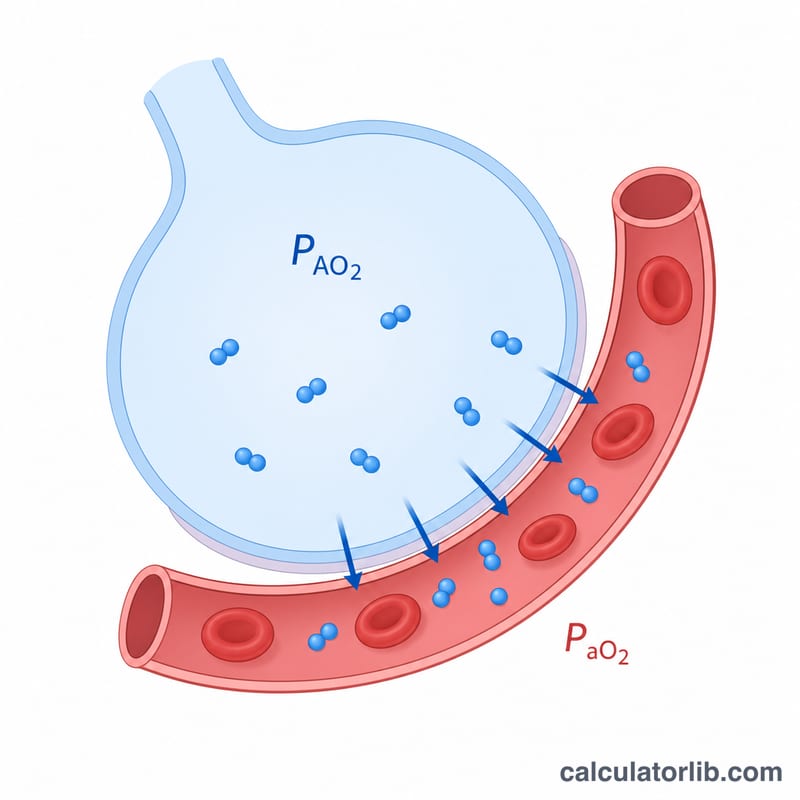
The alveolar–arterial (A-a) oxygen gradient measures the difference between the oxygen concentration in the alveoli (PAO₂) and that in the arterial blood (PaO₂). It is a key tool in assessing the cause of hypoxemia, helping clinicians distinguish between problems of ventilation, diffusion, and gas exchange (such as V/Q mismatch or shunt) versus simple hypoventilation.
How to Use This Calculator
Enter the inspired oxygen fraction (FiO₂, 0.21 for room air), the atmospheric pressure (typically 760 mmHg at sea level), and the arterial blood gas values for PaCO₂ and PaO₂. Optionally enter the patient's age to compute the age-expected normal gradient. The calculator returns the measured A-a gradient, the calculated alveolar oxygen tension, and the expected reference value.
The Formula Explained
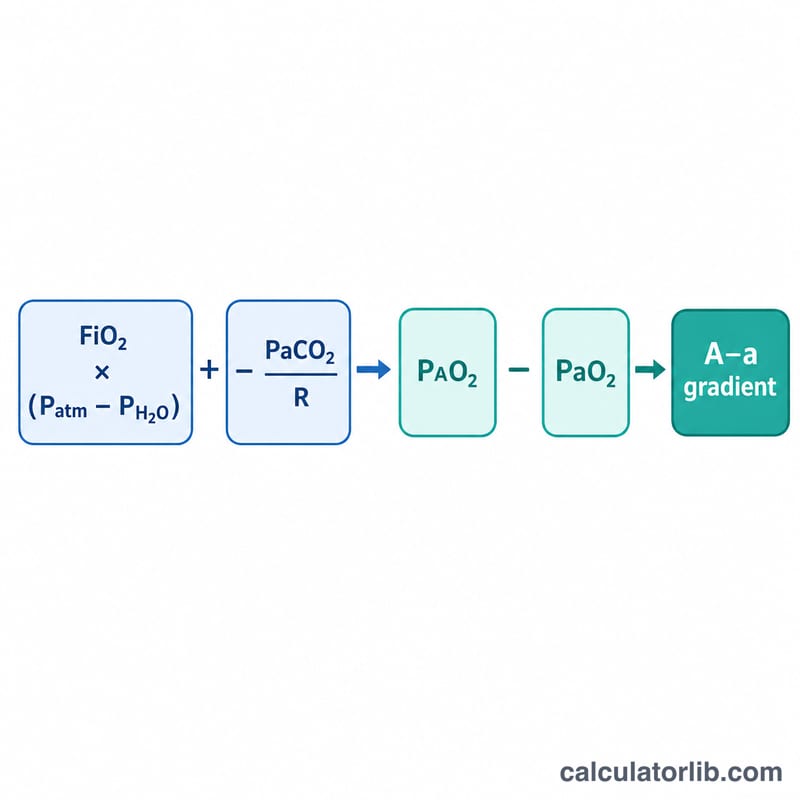
The calculator first solves the alveolar gas equation: $$PAO_2 = FiO_2 \times (P_{atm} - 47) - \dfrac{PaCO_2}{0.8}$$, where 47 mmHg is the partial pressure of water vapor at body temperature and 0.8 is the respiratory quotient (R). The A-a gradient is then \(A\text{-}a = PAO_2 - PaO_2\). A rough age-adjusted upper limit of normal is \(4 + (\text{age} / 4)\) mmHg.
Worked Example
For room air (FiO₂ = 0.21) at 760 mmHg with PaCO₂ = 40 and PaO₂ = 95: $$PAO_2 = 0.21 \times (760 - 47) - \frac{40}{0.8} = 0.21 \times 713 - 50 = 149.73 - 50 = 99.73 \text{ mmHg}$$ The A-a gradient $$A\text{-}a = 99.73 - 95 = 4.73 \text{ mmHg}$$ which is within normal limits for a young adult.
Interpreting Your A-a Gradient
The alveolar–arterial (A-a) oxygen gradient measures the difference between the oxygen tension calculated in the alveoli (\(\text{P}_A\text{O}_2\)) and the oxygen tension measured in arterial blood (\(\text{PaO}_2\)). It is a core part of standard arterial blood gas (ABG) interpretation, used to determine whether hypoxemia originates from a problem with gas exchange across the lung or from another mechanism.
A normal A-a gradient in a hypoxemic patient points toward causes that do not impair the alveolar–capillary interface itself:
- Hypoventilation — for example from sedatives, neuromuscular weakness or central respiratory depression. Here \(\text{PaCO}_2\) rises, \(\text{P}_A\text{O}_2\) falls, and \(\text{PaO}_2\) falls in parallel, so the gradient stays normal.
- Low inspired oxygen (low FiO\(_2\)) — such as at high altitude, where the alveolar oxygen is reduced but gas transfer remains intact.
A widened A-a gradient indicates a defect in oxygen transfer between alveolus and blood. The classic mechanisms are:
- Ventilation–perfusion (V/Q) mismatch — the most common cause, seen in pneumonia, asthma, COPD and pulmonary embolism.
- Right-to-left shunt — blood bypasses ventilated alveoli entirely, as in atelectasis, ARDS, or intracardiac shunts.
- Diffusion impairment — thickening of the alveolar–capillary membrane, as in interstitial lung disease.
A distinguishing feature of a true shunt is that the hypoxemia fails to correct fully with supplemental oxygen. Because shunted blood never contacts alveolar gas, raising FiO\(_2\) cannot oxygenate it, so \(\text{PaO}_2\) rises far less than expected. V/Q mismatch and diffusion limitation, by contrast, typically respond well to increasing FiO\(_2\).
The gradient should always be compared with the age-expected value, since the normal gradient widens with age, and interpreted alongside the full ABG, FiO\(_2\) and clinical picture. This is general educational information and not personal medical advice; clinical decisions should be made by a qualified clinician.
Age-Expected Normal A-a Gradient by Age
The upper limit of a normal A-a gradient rises with age as lung elastic recoil and V/Q matching gradually decline. A common bedside estimate of the expected upper limit (breathing room air) is:
$$\text{Expected} = 4 + \frac{\text{Age}}{4}$$For example, a 60-year-old has an expected upper-limit gradient of \(4 + 60/4 = \) 19 mmHg. The table below applies this formula across common ages.
| Age (years) | Expected upper-limit A-a gradient (mmHg) |
|---|---|
| 20 | 9 |
| 30 | 11.5 |
| 40 | 14 |
| 50 | 16.5 |
| 60 | 19 |
| 70 | 21.5 |
| 80 | 24 |
Values assume the patient is breathing room air (FiO\(_2\) = 0.21). The formula gives an approximate upper bound for a healthy individual; a measured gradient above the age-expected value suggests impaired gas exchange.
Constants Used in the Calculation
The alveolar gas equation behind this calculator relies on several fixed physiologic and physical constants:
| Constant | Symbol | Value | Notes |
|---|---|---|---|
| Water vapor partial pressure | \(\text{P}_{\text{H}_2\text{O}}\) | 47 mmHg | Saturated water vapor pressure at normal body temperature (37 °C); subtracted from atmospheric pressure. |
| Respiratory quotient | R | 0.8 | Ratio of CO\(_2\) produced to O\(_2\) consumed on a typical mixed diet; appears as division of \(\text{PaCO}_2\) by 0.8. |
| Standard atmospheric pressure | \(\text{P}_{atm}\) | 760 mmHg | Barometric pressure at sea level; lower at altitude, which reduces alveolar oxygen. |
| Room-air fraction of inspired oxygen | FiO\(_2\) | 0.21 | Fraction of oxygen in ambient air (about 21%); rises with supplemental oxygen. |
Combining these, the alveolar oxygen tension on room air at sea level is \(\text{P}_A\text{O}_2 = 0.21 \cdot (760 - 47) - \text{PaCO}_2 / 0.8\). With a normal \(\text{PaCO}_2\) of 40 mmHg, this gives \(0.21 \cdot 713 - 50 = 100\) mmHg, the familiar normal alveolar oxygen value.
FAQ
What is a normal A-a gradient? On room air it is roughly 5–10 mmHg in young adults and rises with age (about \(4 + \text{age}/4\) mmHg).
Why does the gradient widen? A widened gradient suggests V/Q mismatch, shunt, or diffusion impairment, whereas a normal gradient with hypoxemia points to hypoventilation or low inspired oxygen.
What pressure should I use at altitude? Use the local barometric pressure; lower atmospheric pressure reduces PAO₂, so this matters for high-altitude assessment.