
What Is the Bicarbonate Deficit Calculator?
This tool estimates the amount of sodium bicarbonate (in milliequivalents, mEq) required to raise a patient's serum bicarbonate (HCO₃⁻) toward a chosen target during metabolic acidosis. It uses the classic bicarbonate space assumption that bicarbonate distributes through roughly 40% of body weight (0.4 L/kg). This is a clinical estimation aid — it does not replace bedside judgment, repeat blood gases, or local protocols.
How to Use It
Enter the patient's body weight in kilograms, the currently measured serum bicarbonate, and the target bicarbonate you want to reach. The calculator returns the total bicarbonate deficit in mEq. Clinicians typically replace only a portion of the deficit initially (often the first half) and then recheck labs before giving more.
The Formula Explained
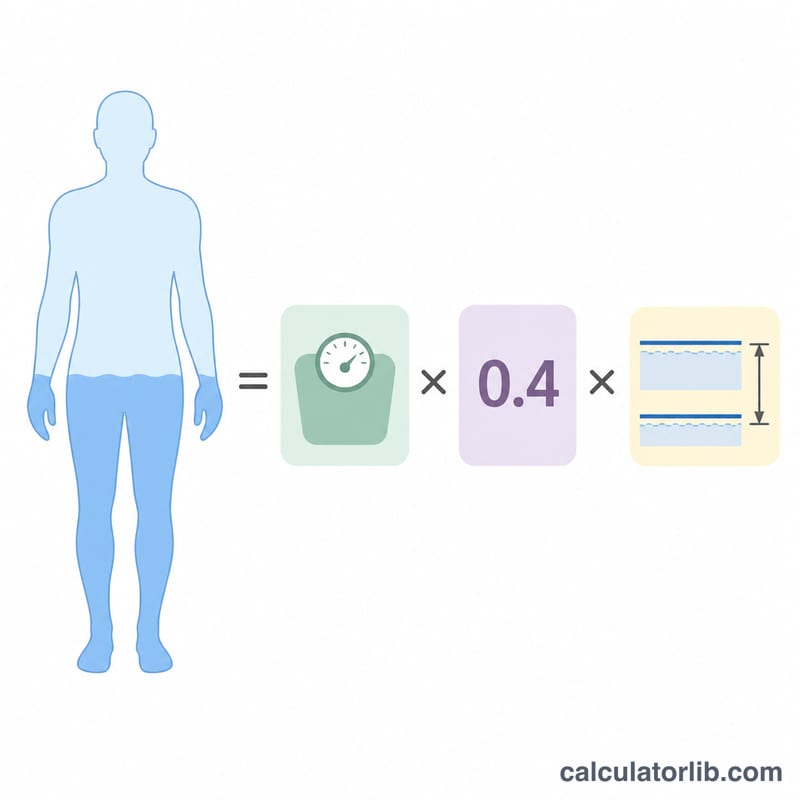
The deficit is calculated as:
$$\text{Deficit (mEq)} = 0.4 \times \text{weight (kg)} \times \left( \text{target HCO}_3^- - \text{measured HCO}_3^- \right)$$
The 0.4 factor represents the apparent volume of distribution of bicarbonate as a fraction of body weight. The distribution space can increase to 0.5–0.8 in severe acidosis, so the 0.4 estimate is conservative and should be paired with clinical reassessment.
Worked Example
A 70 kg patient has a measured HCO₃⁻ of 15 mEq/L and you target 24 mEq/L. $$\text{Deficit} = 0.4 \times 70 \times (24 - 15) = 0.4 \times 70 \times 9 = 252 \text{ mEq}$$ You might administer about half (≈126 mEq) and recheck.
Interpreting Your Result
The number returned is a total estimate of the bicarbonate (in mEq) needed to reach your chosen target — not a single dose to be given all at once. It is a rough guide derived from a population-average distribution space, so the true requirement varies between patients and ongoing acid production (e.g. from sepsis, ketoacidosis, or renal failure) is not accounted for.
A widely used clinical convention is to replace approximately half of the calculated deficit, then recheck an arterial or venous blood gas and electrolytes before giving more. This staged approach lets the body's own buffering and any reversal of the underlying cause contribute, reducing the chance of overshoot.
The factor 0.4 represents bicarbonate's distribution space as a fraction of body weight. In severe acidosis this space expands — values of 0.5 to 0.8 are often cited as HCO₃⁻ falls — so the standard 0.4-based estimate may underestimate the true deficit at very low HCO₃⁻ levels.
Risks of overcorrection include metabolic alkalosis (overshooting pH), hypernatremia and volume overload from the sodium load, hypokalemia, ionized hypocalcemia, and a paradoxical fall in CSF pH. Because of these hazards, slow administration with frequent reassessment is preferred over rapid full correction. The acid–base picture should always be evaluated alongside the anion gap to confirm the type of metabolic acidosis.
This is general information, not professional medical advice. Treatment decisions must be made by a qualified clinician for the individual patient.
Definitions & Glossary
- Bicarbonate (HCO₃⁻)
- The principal buffer base in extracellular fluid and the measured marker of the metabolic component of acid–base balance. A low level indicates metabolic acidosis (or compensation for respiratory alkalosis).
- mEq (milliequivalent)
- A unit of the chemical combining power of an ion. For a monovalent ion such as HCO₃⁻ or Na⁺, 1 mEq equals 1 mmol.
- Metabolic acidosis
- A primary acid–base disturbance characterized by a low serum bicarbonate and a tendency toward a low blood pH, caused by acid accumulation or bicarbonate loss.
- Bicarbonate distribution space
- The effective volume, expressed as a fraction of body weight, through which administered bicarbonate distributes — about 0.4 (40%) under normal conditions but rising to 0.5–0.8 in severe acidosis. It is the multiplier in the deficit formula.
- Deficit
- The estimated total amount of bicarbonate (in mEq) needed to raise the measured serum level to the target, calculated as distribution space × weight × (target − measured).
- Serum (measured) bicarbonate
- The patient's current laboratory HCO₃⁻ value (the actual input), reflecting the present degree of acidosis.
- Target bicarbonate
- The desired HCO₃⁻ level to correct toward (the target input) — commonly a partial goal of ~15 mEq/L or a full goal near the mid-normal value of ~24 mEq/L.
FAQ
Why 0.4? Bicarbonate distributes through about 40% of total body weight under normal conditions; this rises with worsening acidosis.
Should I give the full deficit at once? No. Typically replace partially and recheck arterial or venous blood gases to avoid overcorrection.
Is this calculator country-specific? No — the physiology and formula are universal, though clinical thresholds and protocols vary by institution.