What Is the Anion Gap?
The serum anion gap (AG) is a calculated value that estimates the difference between unmeasured cations and unmeasured anions in the blood. Clinicians use it to help classify metabolic acidosis and to flag the presence of abnormal acids. It is derived from a routine electrolyte panel using sodium, chloride and bicarbonate.
How to Use This Calculator
Enter the patient's serum sodium (Na⁺), chloride (Cl⁻) and bicarbonate (HCO₃⁻) in mEq/L. Optionally enter serum albumin in g/dL to obtain an albumin-corrected anion gap, which is important because low albumin lowers the apparent gap and can mask a true elevation.
The Formula Explained
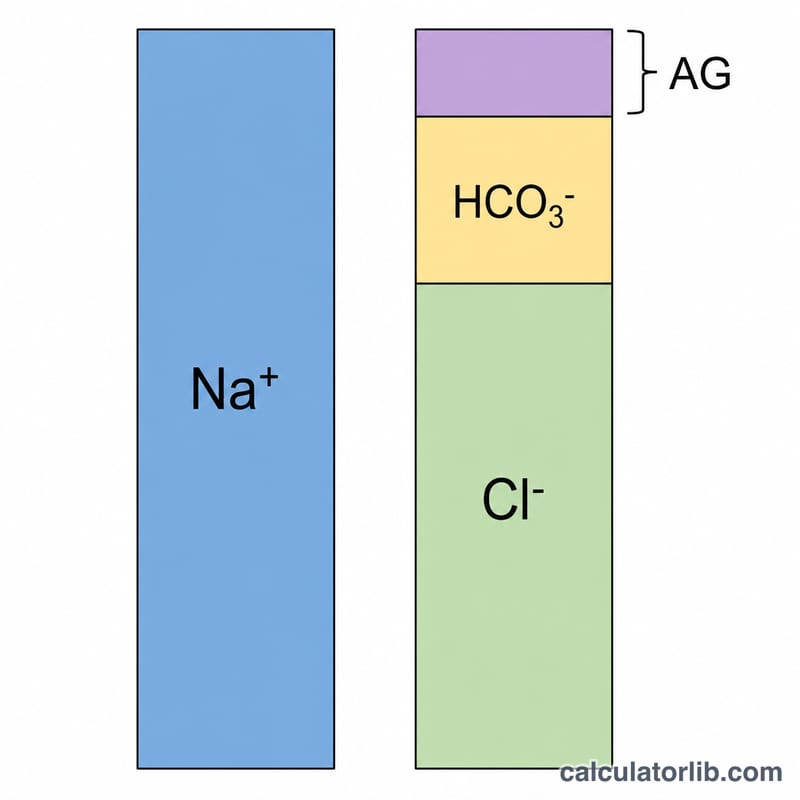
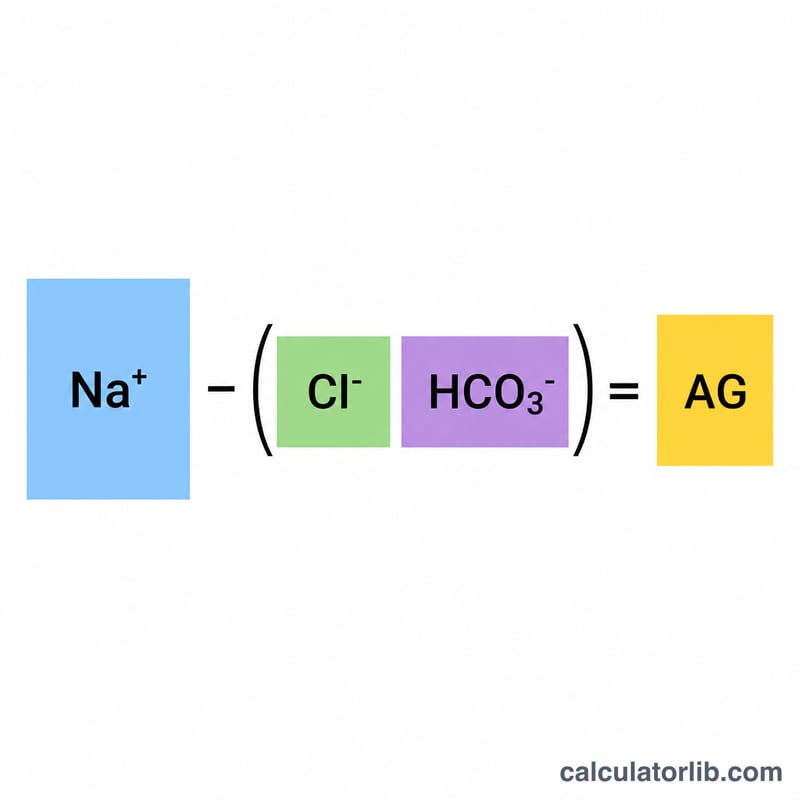
The anion gap is calculated as $$\text{AG} = \text{Na}^{+} - \left( \text{Cl}^{-} + \text{HCO}_3^{-} \right)$$ A normal value is roughly 8–12 mEq/L when potassium is not included. Because albumin is the major unmeasured anion, the corrected gap adds 2.5 mEq/L for every 1 g/dL the albumin falls below 4.0 g/dL: $$\text{AG}_{\text{corr}} = \text{AG} + 2.5 \times \left( 4.0 - \text{albumin} \right)$$
Worked Example
Suppose \(\text{Na}^{+} = 140\), \(\text{Cl}^{-} = 104\) and \(\text{HCO}_3^{-} = 24\) mEq/L. The anion gap is $$140 - (104 + 24) = 140 - 128 = 12 \text{ mEq/L}$$ a normal result. If albumin is 2.0 g/dL, the corrected gap is $$12 + 2.5 \times (4.0 - 2.0) = 12 + 5 = 17 \text{ mEq/L}$$ revealing a high anion gap that the raw value hid.
Interpreting Your Anion Gap Result
The serum anion gap (AG) estimates the unmeasured anions in plasma using \(\text{AG} = \text{Na}^{+} - (\text{Cl}^{-} + \text{HCO}_3^{-})\). It is most useful for narrowing the differential diagnosis of a metabolic acidosis, but the number must always be interpreted alongside the clinical picture, the bicarbonate level, and the serum albumin.
What the result indicates
- High anion gap (>12 mEq/L) suggests accumulation of unmeasured anions. In the setting of a low bicarbonate this defines a high anion gap metabolic acidosis (HAGMA) — for example a patient with \(\text{Na}^{+}=140\), \(\text{Cl}^{-}=100\), \(\text{HCO}_3^{-}=12\) has an AG of 28 mEq/L.
- Normal anion gap (8–12 mEq/L) with a low bicarbonate points to a normal anion gap (hyperchloremic) metabolic acidosis (NAGMA), where bicarbonate loss is matched by a rise in chloride.
- Low anion gap (<3–6 mEq/L) is uncommon and usually reflects laboratory or protein causes rather than acid–base disease.
HAGMA vs NAGMA
The key branch point in a metabolic acidosis is whether the gap is elevated. A widened gap (HAGMA) means an acid with an unmeasured anion has been added. A normal gap (NAGMA) means bicarbonate has been lost (gastrointestinal or renal) and replaced by chloride.
Common mnemonics
- High-gap causes — MUDPILES: Methanol, Uremia, Diabetic (and other) ketoacidosis, Propylene glycol/Paraldehyde, Iron/Isoniazid, Lactic acidosis, Ethylene glycol, Salicylates.
- Normal-gap causes — HARDASS: Hyperalimentation, Acetazolamide, Renal tubular acidosis, Diarrhea, Addison disease, Spironolactone, Saline (excess). The mnemonic GOLD MARK (Glycols, Oxoproline, L-lactate, D-lactate, Methanol, Aspirin, Renal failure, Ketoacidosis) is a more modern list for high-gap causes.
Low-gap causes
A low anion gap most often results from hypoalbuminemia (albumin is the dominant unmeasured anion), and less commonly from cationic paraproteins (e.g. some plasma cell dyscrasias), lithium toxicity, severe hypercalcemia or hypermagnesemia, or bromide/iodide interference. Because each 1 g/dL fall in albumin lowers the apparent gap by about 2.5 mEq/L, a “normal” gap in a hypoalbuminemic patient may actually be elevated once corrected.
This is general educational information, not medical advice. Anion gap values must be interpreted by a qualified clinician in the context of the full clinical assessment.
Anion Gap Reference Values
Reference ranges vary slightly between laboratories and depend on whether potassium is included in the calculation. The values below are widely cited approximate ranges.
| Category | Without K⁺ (Na − [Cl + HCO₃]) | With K⁺ ([Na + K] − [Cl + HCO₃]) |
|---|---|---|
| Normal | 8–12 mEq/L | 12–16 mEq/L |
| Elevated (high gap) | > 12 mEq/L | > 16 mEq/L |
| Low | < 3–6 mEq/L | < 6–8 mEq/L |
Albumin correction
Albumin is the largest contributor to the normal anion gap, so hypoalbuminemia lowers the measured gap and can mask a true elevation. The corrected anion gap adds back roughly 2.5 mEq/L for every 1 g/dL the albumin sits below 4.0 g/dL:
$$\text{Corrected AG} = \text{AG} + 2.5 \times (4.0 - \text{albumin in g/dL})$$
| Parameter | Reference value |
|---|---|
| Normal serum albumin | 3.5–5.0 g/dL |
| Correction factor | 2.5 mEq/L per 1 g/dL below 4.0 g/dL |
| Reference albumin used | 4.0 g/dL |
Use your own laboratory’s reference interval where available; some labs report a narrower normal range (e.g. 3–11 mEq/L) due to modern ion-selective electrodes.
Anion Gap Across Common Scenarios
The table illustrates how the same formula yields different classifications, and how the albumin correction can unmask an elevated gap that the raw value misses. Raw AG uses \(\text{Na}^{+} - (\text{Cl}^{-} + \text{HCO}_3^{-})\); corrected AG adds \(2.5 \times (4.0 - \text{albumin})\).
| Scenario | Na⁺ (mEq/L) | Cl⁻ (mEq/L) | HCO₃⁻ (mEq/L) | Albumin (g/dL) | Raw AG | Corrected AG | Classification |
|---|---|---|---|---|---|---|---|
| Normal | 140 | 104 | 24 | 4.0 | 12 | 12 | Normal gap |
| High-gap acidosis (e.g. DKA) | 138 | 100 | 10 | 4.0 | 28 | 28 | HAGMA |
| Hypoalbuminemia masking elevation | 138 | 108 | 18 | 2.0 | 12 | 17 | True high gap (unmasked) |
| Normal-gap acidosis (e.g. diarrhea) | 140 | 116 | 14 | 4.0 | 10 | 10 | NAGMA |
The third row is the key teaching point: a raw gap of 12 looks normal, but with an albumin of 2.0 g/dL the correction adds \(2.5 \times (4.0 - 2.0) = 5\) mEq/L, giving a corrected gap of 17 mEq/L and revealing a genuine high-gap process. In acid–base assessment this AG is often combined with a serum osmolality estimate when toxic alcohol ingestion is suspected.
FAQ
Should I include potassium? This calculator uses the common \(\text{Na} - (\text{Cl} + \text{HCO}_3)\) formula without potassium. Including K⁺ raises the normal range by about 4 mEq/L.
What causes a high anion gap? Lactic acidosis, ketoacidosis, renal failure and certain toxins (e.g., methanol, ethylene glycol, salicylates).
Is this medical advice? No. This tool is for educational and informational purposes and should be interpreted by a qualified clinician.