What Is the Anion Gap?
The anion gap (AG) is a calculated value derived from a basic metabolic panel that estimates the difference between unmeasured anions and cations in the blood. It is a cornerstone of acid-base assessment, helping clinicians classify metabolic acidosis as either high-anion-gap or normal-anion-gap. This calculator is intended for educational reference; it is not a substitute for clinical judgment.
How to Use It
Enter the patient's serum sodium (Na+), chloride (Cl-) and bicarbonate (HCO3-) values in mmol/L. Optionally enter serum albumin in g/dL to compute the albumin-corrected anion gap. The default albumin of 4.0 g/dL leaves the gap unchanged. Results display the raw serum anion gap and the corrected value.
The Formula Explained
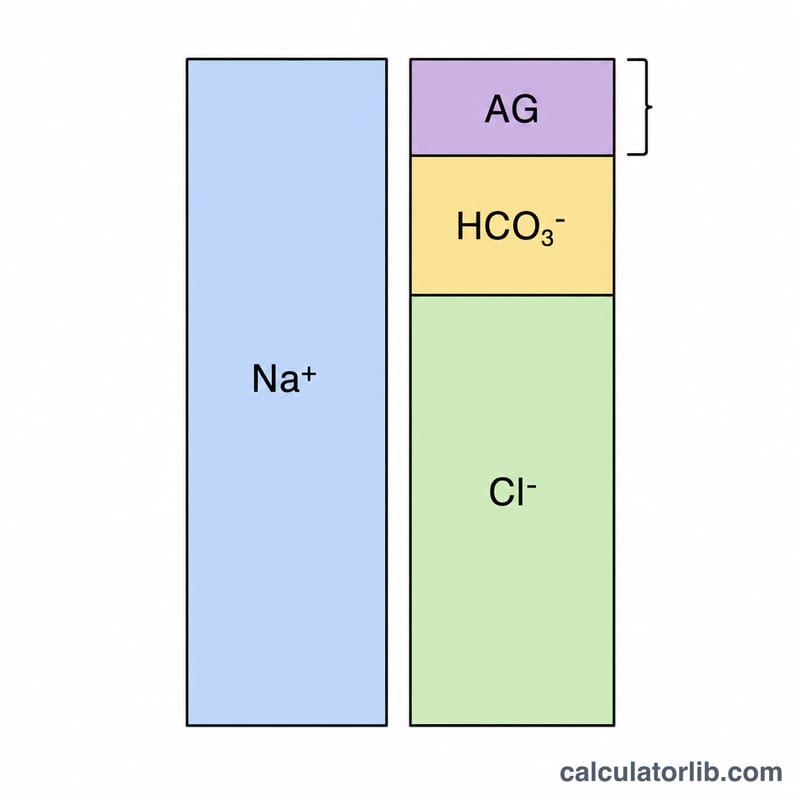
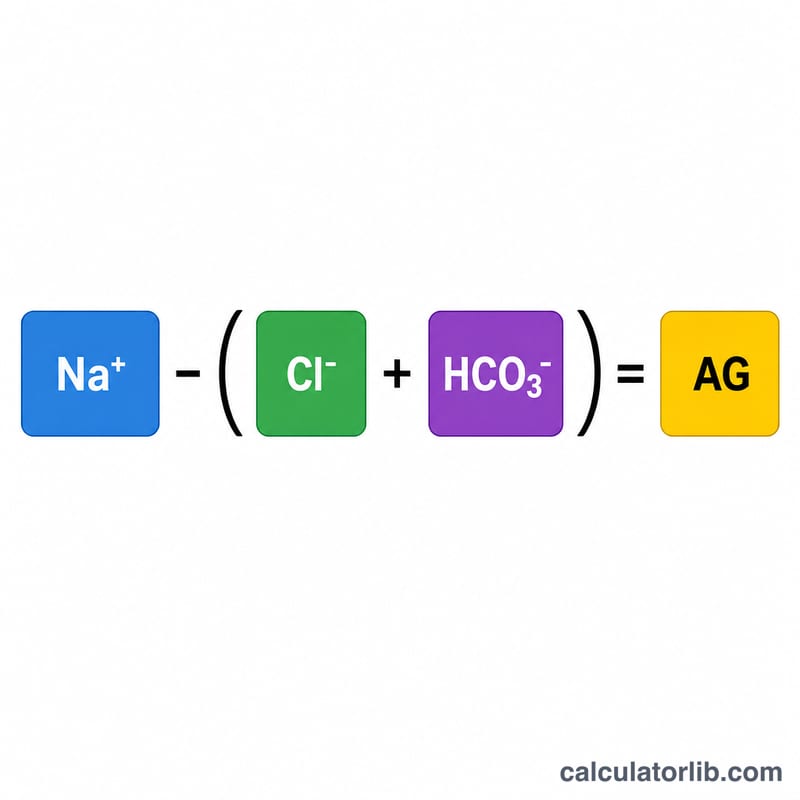
The basic anion gap is \( \text{AG} = \text{Na}^{+} - (\text{Cl}^{-} + \text{HCO}_3^{-}) \). Potassium is usually omitted because it changes little. A normal anion gap is roughly 8–12 mmol/L (varies by lab and whether potassium is included). Because albumin is the major unmeasured anion, hypoalbuminemia lowers the apparent gap; the correction adds 2.5 mmol/L for every 1 g/dL the albumin falls below 4.0 g/dL: \( \text{cAG} = \text{AG} + 2.5 \times (4.0 - \text{albumin}) \).
Worked Example
For Na+ = 140, Cl− = 104, HCO3− = 24, albumin = 3.0:
$$\text{AG} = 140 - (104 + 24) = 12 \text{ mmol/L}$$Corrected:
$$\text{cAG} = 12 + 2.5 \times (4.0 - 3.0) = 12 + 2.5 = 14.5 \text{ mmol/L}$$The correction reveals a higher effective gap than the raw value suggests.
Interpreting Your Anion Gap Result
The anion gap (AG) estimates the difference between routinely measured cations and anions in serum. It is a screening tool that helps classify metabolic acidosis and flag the presence of unmeasured anions. Both the raw value and the albumin-corrected value should be considered, because low albumin can mask a true elevation.
Using the common reference of Na⁺ minus (Cl⁻ + HCO₃⁻), a result above roughly 12 mmol/L is generally considered a high anion gap. A high gap reflects accumulation of unmeasured acids — most often lactate (lactic acidosis), ketoacids (diabetic, alcoholic, or starvation ketoacidosis), retained acids in renal failure, or ingested toxins (methanol, ethylene glycol, salicylates). The MUDPILES mnemonic is widely used to recall these causes.
A normal anion gap acidosis (also called hyperchloremic acidosis) occurs when bicarbonate is lost or chloride is retained without added organic acids — classic causes include diarrhea, renal tubular acidosis (RTA), and certain medications. Here the gap stays within range while bicarbonate falls and chloride rises.
A low anion gap (below about 8 mmol/L) is uncommon and most often reflects hypoalbuminemia, since albumin is the dominant unmeasured anion. Other causes include paraproteins (e.g., certain myelomas), lithium excess, severe hypercalcemia, or laboratory artifact. Because albumin contributes about 2.5 mmol/L of gap per 1 g/dL, the corrected anion gap adds 2.5 × (4.0 − measured albumin) to unmask a hidden elevated gap in low-albumin patients.
In high-gap acidosis, clinicians also assess the delta-delta (delta ratio): comparing the rise in anion gap to the fall in bicarbonate helps detect a coexisting normal-gap acidosis or metabolic alkalosis. A roughly 1:1 change suggests a pure high-gap process, while disproportionate changes point to a mixed disorder.
All thresholds are lab- and method-dependent (whether potassium is included, the analyzer used, and the local reference interval), so interpret your value against your laboratory's stated range and the full clinical picture. This is general educational information, not medical advice; discuss any result with a qualified clinician.
Anion Gap Reference Ranges
The following ranges use the standard formula AG = Na⁺ − (Cl⁻ + HCO₃⁻). Many laboratories now report a normal range of roughly 8–12 mmol/L because current ion-selective electrode methods read chloride slightly higher than older techniques. When potassium is added to the cation side, the normal range shifts upward (about 12–16 mmol/L).
| Category | AG (Na only, mmol/L) | Interpretation |
|---|---|---|
| Low | < 8 | Often hypoalbuminemia, paraproteins, lithium, severe hypercalcemia, or artifact |
| Normal | 8 – 12 | Typical reference interval (12–16 if potassium included) |
| Borderline high | 12 – 16 | Possible mild elevation; correlate with albumin and clinical context |
| High | > 12 | Suggests unmeasured acids (lactate, ketones, renal, toxins) |
| Severely high | > 20 | Strongly indicates significant high-gap metabolic acidosis |
After albumin correction, the expected normal value centers around 12 mmol/L. Because every laboratory calibrates its electrolyte assays differently, always compare your result to the reference range printed on your own lab report rather than to a single universal cutoff.
Key Terms and Variables
- Sodium (Na⁺)
- The principal measured cation in serum and the only cation used in the basic anion gap formula. Reported in mmol/L (equivalent to mEq/L for monovalent ions).
- Chloride (Cl⁻)
- The major measured anion. A relative rise in chloride alongside a falling bicarbonate is the hallmark of normal-gap (hyperchloremic) acidosis.
- Bicarbonate (HCO₃⁻)
- The measured buffer anion (total CO₂ on many panels). Its loss or consumption drives metabolic acidosis.
- Albumin
- The dominant unmeasured anion under physiologic conditions, normally about 4.0 g/dL. Low albumin lowers the measured gap and must be corrected for.
- Anion gap (AG)
- The calculated difference between measured cations and measured anions: AG = Na⁺ − (Cl⁻ + HCO₃⁻). It represents the unmeasured anions exceeding unmeasured cations.
- Corrected anion gap
- The AG adjusted for albumin: AG + 2.5 × (4.0 − albumin in g/dL). Reveals a true elevation hidden by hypoalbuminemia.
- Unmeasured anions / cations
- Charged species not on the basic panel — anions include albumin, phosphate, sulfate, lactate, and ketoacids; cations include potassium, calcium, and magnesium.
- Metabolic acidosis
- A primary fall in serum bicarbonate with reduced blood pH, subdivided by the anion gap.
- High-anion-gap acidosis
- Acidosis from added organic or fixed acids that consume bicarbonate while chloride stays unchanged, raising the gap.
- Normal-anion-gap acidosis
- Acidosis from bicarbonate loss with compensatory chloride retention; the gap remains within range (hyperchloremic acidosis).
- MUDPILES
- A mnemonic for high-gap causes: Methanol, Uremia, Diabetic ketoacidosis, Propylene glycol (or Paraldehyde), Iron/Isoniazid, Lactic acidosis, Ethylene glycol, Salicylates.
FAQ
Why correct for albumin? Low albumin masks an elevated anion gap, so a "normal" raw gap may actually be high once corrected.
Should I include potassium? Some labs use Na+ + K+ in the formula, raising the normal range to about 12–16 mmol/L. This tool uses the common sodium-only version.
What does a high anion gap suggest? Causes include lactic acidosis, ketoacidosis, renal failure, and certain toxins (often recalled by the mnemonic MUDPILES).