
What is the Alvarado Score?
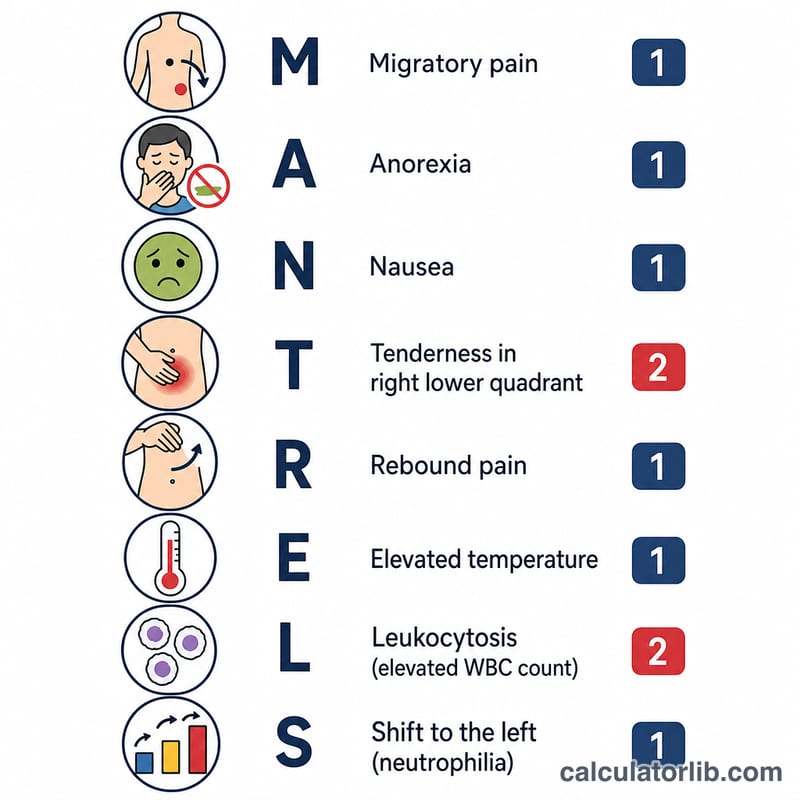
The Alvarado Score is a clinical scoring system used to estimate the likelihood of acute appendicitis in patients presenting with abdominal pain. It combines patient symptoms, physical examination signs, and two laboratory findings into a single number from 0 to 10. The mnemonic MANTRELS captures the eight components: Migration of pain, Anorexia, Nausea/vomiting, Tenderness in the right lower quadrant, Rebound pain, Elevated temperature, Leukocytosis, and Shift of neutrophils to the left.
How to use this calculator
Answer each of the eight items based on the patient's history, examination, and complete blood count. Most items add 1 point when present; right lower quadrant tenderness and leukocytosis (white cell count ≥ 10,000/mm³) each add 2 points because they are the strongest predictors. The calculator totals the points and gives a risk interpretation.
The formula explained
$$\text{Score} = M + A + N + 2T + R + E + 2L + S$$
Score = Migration(1) + Anorexia(1) + Nausea(1) + RLQ tenderness(2) + Rebound(1) + Fever ≥ 37.3 °C (1) + Leukocytosis (2) + Left shift ≥ 75% neutrophils (1), to a maximum of 10. A common interpretation: 1–4 = unlikely, 5–6 = possible (observe or image), 7–10 = probable appendicitis (surgical consultation).
Worked example
A patient has migration of pain (1), anorexia (1), nausea (1), right lower quadrant tenderness (2), rebound (1), no fever (0), WBC of 12,500/mm³ → leukocytosis (2), and neutrophils 60% → no left shift (0). Total = \(1+1+1+2+1+0+2+0 = 8\), indicating a high probability of appendicitis.
Interpreting Your Alvarado Score
The Alvarado (MANTRELS) score sums eight clinical and laboratory findings into a single value from 0 to 10. The total is conventionally grouped into three risk bands that guide how clinicians approach a patient with suspected acute appendicitis. Higher scores correspond to a greater probability that appendicitis is the true cause of the patient's presentation.
| Score | Risk band | Approximate likelihood of appendicitis | Typical management implication |
|---|---|---|---|
| 0–4 | Low / unlikely | Appendicitis improbable; negative predictive value is high in this range | Appendicitis can usually be reasonably excluded; supports discharge with safety-netting or brief observation rather than imaging or surgery |
| 5–6 | Intermediate / possible | Appendicitis cannot be confidently confirmed or excluded | Favors continued observation, serial reassessment, and/or cross-sectional imaging (commonly ultrasound or CT) before a decision |
| 7–10 | High / probable | High positive predictive value; appendicitis is the most likely diagnosis | Supports surgical consultation; some pathways proceed toward appendectomy, others image first depending on patient and institution |
The Alvarado score was originally derived with a recommended threshold of \(\geq 7\) to prompt surgical evaluation. Subsequent validation studies have shown the score performs well at ruling appendicitis out at low values but is less reliable for ruling it in, and its discriminatory performance varies by sex and age (for example, it tends to over-predict in women). For this reason it is used as a decision-support aid alongside history, repeat examination, and imaging — not as a stand-alone diagnostic test.
This information is general and educational only. It is not a substitute for evaluation by a qualified clinician, and no score should be used to self-diagnose or to delay seeking care for severe or worsening abdominal pain.
FAQ
Is the Alvarado Score diagnostic? No. It is a risk-stratification aid, not a definitive diagnosis. It should be combined with clinical judgment and imaging when indicated.
What cut-off should I use? Many centers use ≥ 7 to suggest likely appendicitis, but local protocols vary; a Modified Alvarado Score drops the left-shift item for a maximum of 9.
Does it work for everyone? Performance differs in women, children, and the elderly. Always interpret in clinical context.