What Is the Albumin-to-Creatinine Ratio (ACR)?
The urine albumin-to-creatinine ratio (ACR) is a widely used screening test for kidney damage. By measuring how much albumin (a protein) appears in the urine relative to creatinine, the test corrects for how dilute or concentrated a single "spot" urine sample is. This makes a random sample almost as reliable as a cumbersome 24-hour collection. ACR is a core measure in the KDIGO classification of chronic kidney disease (CKD).
How to Use This Calculator
Enter your urine albumin concentration and urine creatinine concentration, both reported in mg/dL (the typical units on a lab panel). The calculator divides albumin by creatinine and multiplies by 1000 to express the result in milligrams of albumin per gram of creatinine (mg/g). It also classifies the value into KDIGO albuminuria stages.
The Formula Explained
The equation is: $$\text{ACR (mg/g)} = \dfrac{\text{Urine Albumin (mg/dL)}}{\text{Urine Creatinine (mg/dL)}} \times 1000$$ The factor of 1000 converts the per-deciliter ratio into the standard per-gram-of-creatinine reporting unit, because 1 gram = 1000 milligrams. Higher ACR values indicate more albumin leaking into the urine.
Worked Example
Suppose a urine sample shows albumin of 3 mg/dL and creatinine of 100 mg/dL. $$\text{ACR} = \left(\frac{3}{100}\right) \times 1000 = 30 \text{ mg/g}$$ A value of 30 mg/g sits at the border of the moderately increased (A2) category.
Interpreting Your ACR Result
The ACR estimates how much albumin (a protein) is leaking from the blood into the urine, which can be an early marker of kidney damage. Each KDIGO category carries a different general meaning:
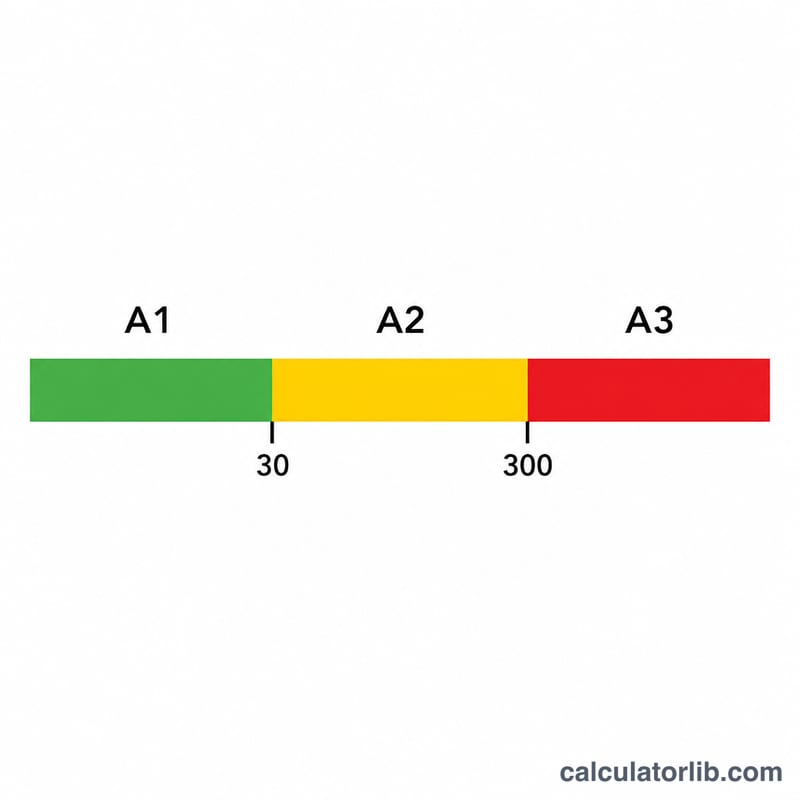
- A1 (< 30 mg/g): Albumin excretion is within the normal to mildly increased range. This is the expected result for most people without kidney disease.
- A2 (30–300 mg/g): Moderately increased albuminuria. This can be an early sign of kidney damage and is often monitored in people with diabetes or high blood pressure.
- A3 (> 300 mg/g): Severely increased albuminuria, indicating more significant protein loss and a higher risk of kidney disease progression.
Confirmation and persistence. A single elevated ACR does not establish chronic kidney disease. Albuminuria should be persistent: KDIGO considers it confirmed when at least 2 of 3 samples collected over roughly 3 months are abnormal. A preferred first-morning (early-morning) urine sample reduces variability.
Transient elevations. Several non-kidney factors can temporarily raise the ACR, including recent vigorous exercise, fever, urinary tract or other infection, menstrual blood contamination, marked hyperglycemia, heart failure, and very high protein intake. Repeat testing when these factors have resolved gives a more reliable result.
Use with eGFR. ACR measures kidney damage, while eGFR measures kidney function — the two are complementary, and KDIGO staging uses both together. ACR is frequently interpreted alongside an eGFR value to give the full “G–A” CKD stage.
This information is general and educational only and is not medical advice. Discuss your results and any next steps with a qualified healthcare professional.
ACR Unit Conversion (mg/g ↔ mg/mmol)
ACR is reported in mg/g (common in the United States) or in mg/mmol (common in many other countries and SI laboratories). The two scales differ by the molar mass of creatinine (about 113 g/mol), giving the practical conversion factor:
$$\text{ACR (mg/mmol)} = \frac{\text{ACR (mg/g)}}{8.84}$$Equivalently, multiply mg/mmol by 8.84 to obtain mg/g. The table below shows the KDIGO threshold values and a few common points.
| ACR (mg/g) | ACR (mg/mmol) | KDIGO category |
|---|---|---|
| 10 | ≈ 1.1 | A1 |
| 30 | ≈ 3.4 | A1 → A2 boundary |
| 100 | ≈ 11.3 | A2 |
| 300 | ≈ 34 | A2 → A3 boundary |
| 1000 | ≈ 113 | A3 |
Worked example: \(300 \div 8.84 = 33.9 \approx 34\) mg/mmol, and \(30 \div 8.84 = 3.39 \approx 3.4\) mg/mmol — matching the standard A2 and A3 cut points.
FAQ
What is a normal ACR? Below 30 mg/g is considered normal to mildly increased (A1). 30–300 mg/g is moderately increased (A2), and above 300 mg/g is severely increased (A3).
Does the time of day matter? A first-morning sample is preferred because it reduces variability, but a random spot sample is acceptable for screening.
Is this a diagnosis? No. ACR is a screening tool. Always discuss results with a healthcare professional, as factors like exercise, fever, and infection can temporarily raise albumin.