What is sodium correction for hyperglycemia?
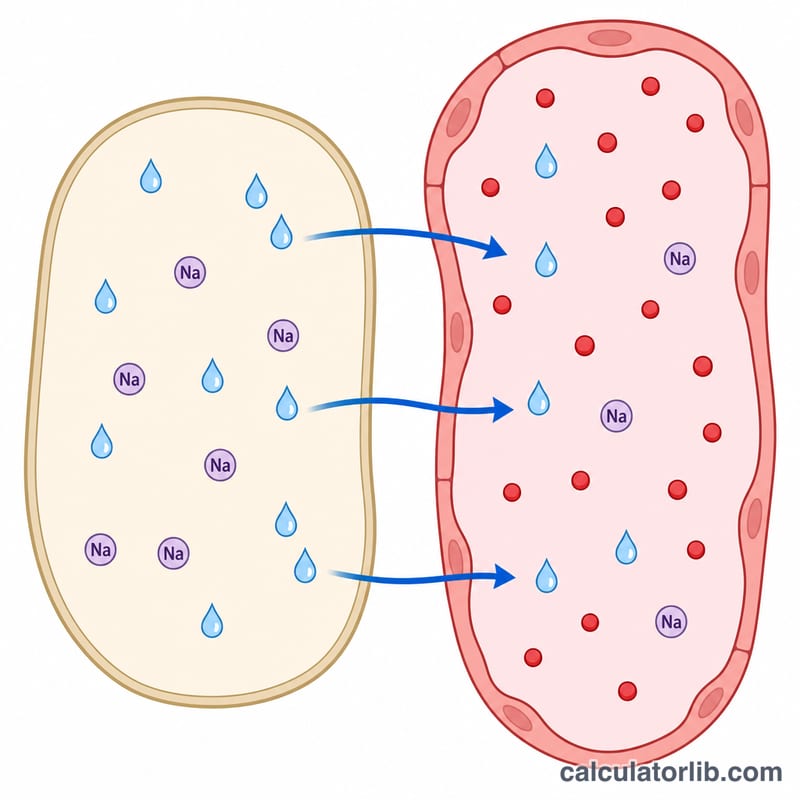
When blood glucose is high, water is osmotically pulled from cells into the bloodstream, diluting the serum sodium and producing a falsely low (pseudohyponatremic) measured value. The sodium correction for hyperglycemia formula estimates what the sodium would be if glucose were normal, helping clinicians judge a patient's true sodium and fluid status. This tool is a general educational reference and is not a substitute for clinical judgment.
How to use this calculator
Enter the laboratory-measured serum sodium in mEq/L and the serum glucose in mg/dL. The calculator returns the corrected sodium, the amount of correction added, and the inputs for reference. It is most useful when glucose exceeds 100 mg/dL; below that the correction becomes negative and is generally not clinically relevant.
The formula explained
This calculator uses the commonly cited correction factor of 0.016:
$$\text{Na}_{corrected} = \text{Measured Na} + 0.016 \times \left( \text{Glucose} - 100 \right)$$
For each 1 mg/dL the glucose sits above the reference 100 mg/dL, 0.016 mEq/L is added back to the measured sodium. This equals roughly 1.6 mEq/L per 100 mg/dL of glucose. Some authors prefer a 0.024 factor (about 2.4 mEq/L per 100 mg/dL), which may be more accurate at very high glucose levels.
Worked example
A patient has a measured sodium of 130 mEq/L and a glucose of 600 mg/dL. Correction $$= 0.016 \times \left( 600 - 100 \right) = 0.016 \times 500 = 8 \text{ mEq/L}.$$ Corrected sodium $$= 130 + 8 = 138 \text{ mEq/L}.$$ The apparent hyponatremia is explained by hyperglycemia; the true sodium is normal.
FAQ
Why subtract 100? 100 mg/dL approximates a normal fasting glucose; correction is applied only for glucose above this baseline.
Which factor is correct, 0.016 or 0.024? Both are used. The classic 1.6 mEq/L (0.016) factor is most widely taught; the 2.4 factor may better match measured values when glucose is very high.
What sodium guides treatment? The corrected sodium reflects true sodium status, while the measured value reflects the osmotic dilution. Both should be interpreted with the full clinical picture.