What Is the Corrected Sodium Calculator?
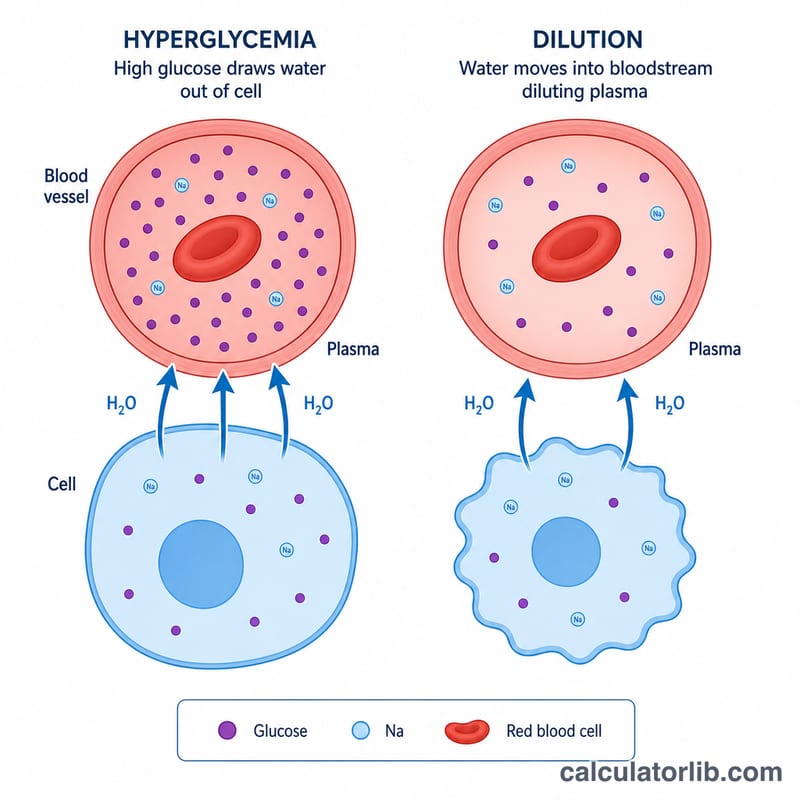
High blood glucose draws water out of cells into the bloodstream, diluting the serum sodium and producing a falsely low measured value (pseudohyponatremia/dilutional hyponatremia). This calculator estimates what the serum sodium would be if the glucose were normal, helping clinicians judge a patient's true sodium status during hyperglycemia or diabetic ketoacidosis (DKA). It is intended for clinical education and quick bedside estimation, not as a substitute for professional judgment.
How to Use It
Enter the laboratory-measured serum sodium (mEq/L) and the blood glucose (mg/dL). Choose a correction factor: the classic 1.6 (Katz) is most widely taught, while 2.4 (Hillier et al.) better fits glucose levels above ~400 mg/dL. The tool returns the corrected sodium and the amount added.
The Formula Explained
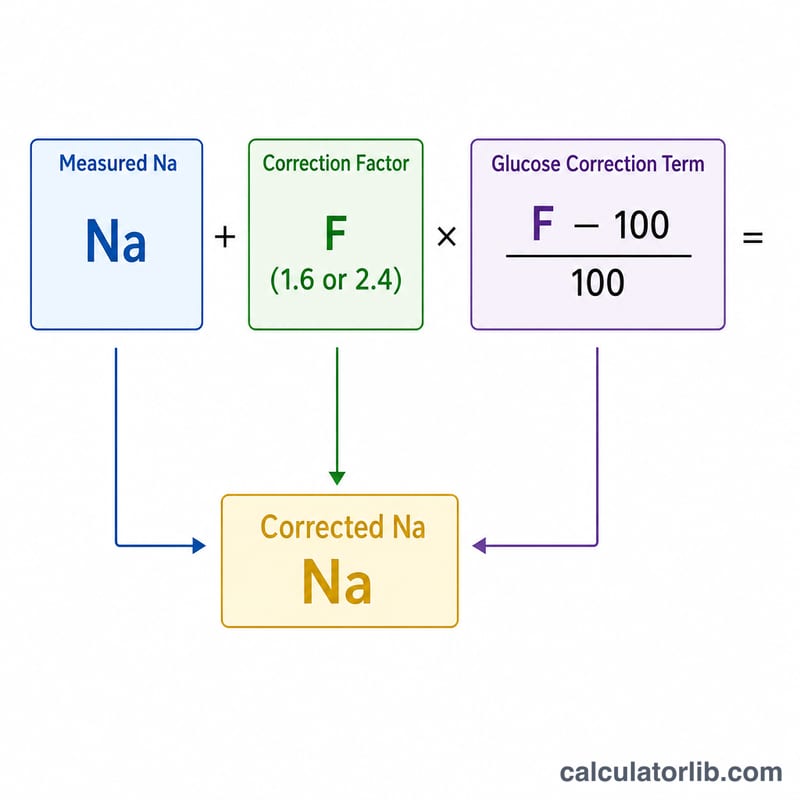
$$\text{Na}_{corrected} = \text{Measured Na} + F \times \frac{\text{Glucose} - 100}{100}$$ where \(F\) is 1.6 or 2.4. For every 100 mg/dL that glucose exceeds 100 mg/dL, the correction factor is added to the measured sodium. When glucose is at or below 100 mg/dL, no correction is needed.
Worked Example
A patient in DKA has a measured sodium of 130 mEq/L and glucose of 500 mg/dL. Using the 1.6 factor: $$\text{correction} = 1.6 \times \frac{500 - 100}{100} = 1.6 \times 4 = 6.4 \text{ mEq/L}$$ $$\text{Corrected Na} = 130 + 6.4 = 136.4 \text{ mEq/L}$$ — a normal value, revealing the apparent hyponatremia is dilutional.
FAQ
Should I use 1.6 or 2.4? Use 1.6 for general estimation; 2.4 may be more accurate when glucose exceeds 400 mg/dL.
What if glucose is below 100? The correction becomes negative or zero; no correction is generally applied below 100 mg/dL.
Why does the measured sodium look low? Osmotic shift of water from cells dilutes plasma sodium; correcting reveals the true sodium and guides fluid therapy.