What is the Wells Score for Pulmonary Embolism?
The Wells Score for pulmonary embolism (PE) is a validated clinical prediction rule that estimates the pretest probability that a patient has a PE. It combines seven weighted clinical criteria into a single point total, helping clinicians decide whether to order a D-dimer test, proceed to CT pulmonary angiography, or pursue other diagnostics. This tool is a decision-support aid only and does not replace clinical judgment.
How to use the calculator
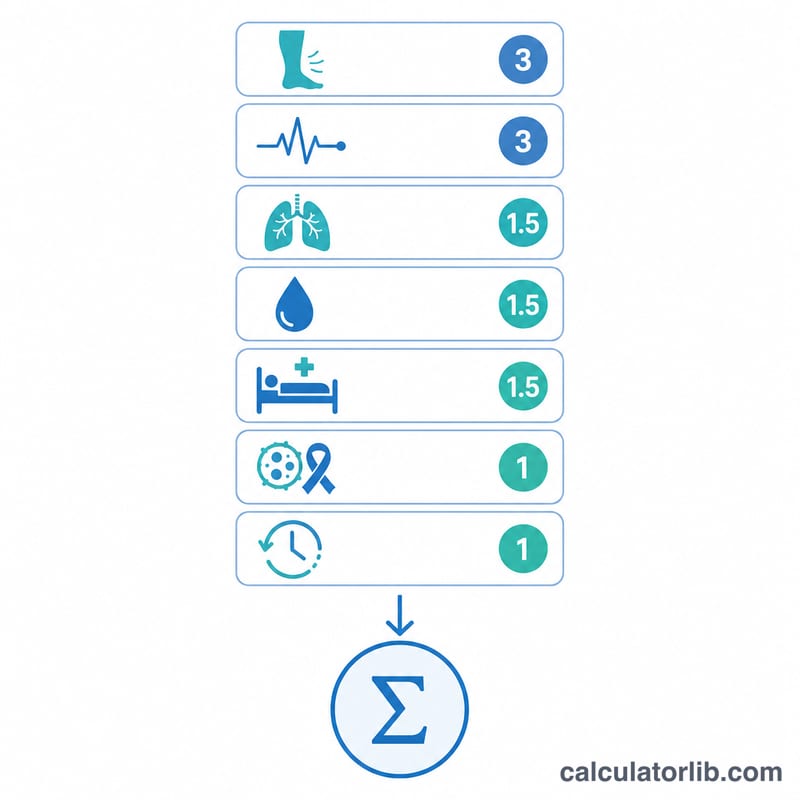
Check each criterion that applies to your patient. Each box carries a fixed weight: clinical signs of DVT (+3.0), PE being the most likely diagnosis (+3.0), heart rate above 100 bpm (+1.5), immobilization or recent surgery (+1.5), prior PE/DVT (+1.5), hemoptysis (+1.0), and active malignancy (+1.0). The calculator sums the points and returns both interpretation schemes instantly.
The formula explained
The total is simply the sum of the weighted criteria.
$$\text{Score} = 3.0\,\text{Signs of DVT} + 3.0\,\text{PE most likely} + 1.5\,\text{HR} > 100 + 1.5\,\text{Immobilization} + 1.5\,\text{Prior PE/DVT} + 1.0\,\text{Hemoptysis} + 1.0\,\text{Malignancy}$$
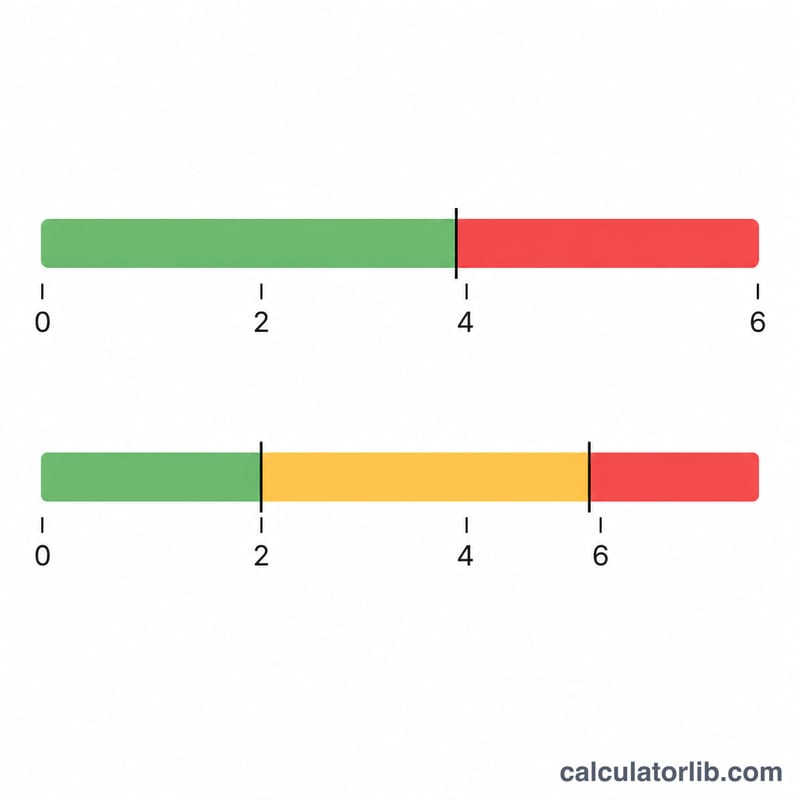
The original three-tier model classifies a score of 0–1 as low risk, 2–6 as moderate risk, and ≥7 as high risk. The widely used two-tier (dichotomized) model labels a score of ≤4 as "PE unlikely" and >4 as "PE likely." In the unlikely group, a negative D-dimer can often safely rule out PE.
Worked example
A patient has clinical signs of DVT (+3.0), a heart rate of 110 bpm (+1.5), and hemoptysis (+1.0). The total is $$3.0 + 1.5 + 1.0 = 5.5 \text{ points}.$$ That places them in the moderate three-tier category and the "PE likely" two-tier category, suggesting imaging rather than D-dimer alone.
FAQ
Two-tier or three-tier? The two-tier model is now more common because it pairs cleanly with D-dimer testing. Both are reported here.
What if the total is exactly 4? A score of 4 falls in the "PE unlikely" group (the cutoff is >4 for "likely").
Is this diagnostic? No. The Wells Score estimates probability to guide testing; only imaging or further workup can confirm or exclude PE.